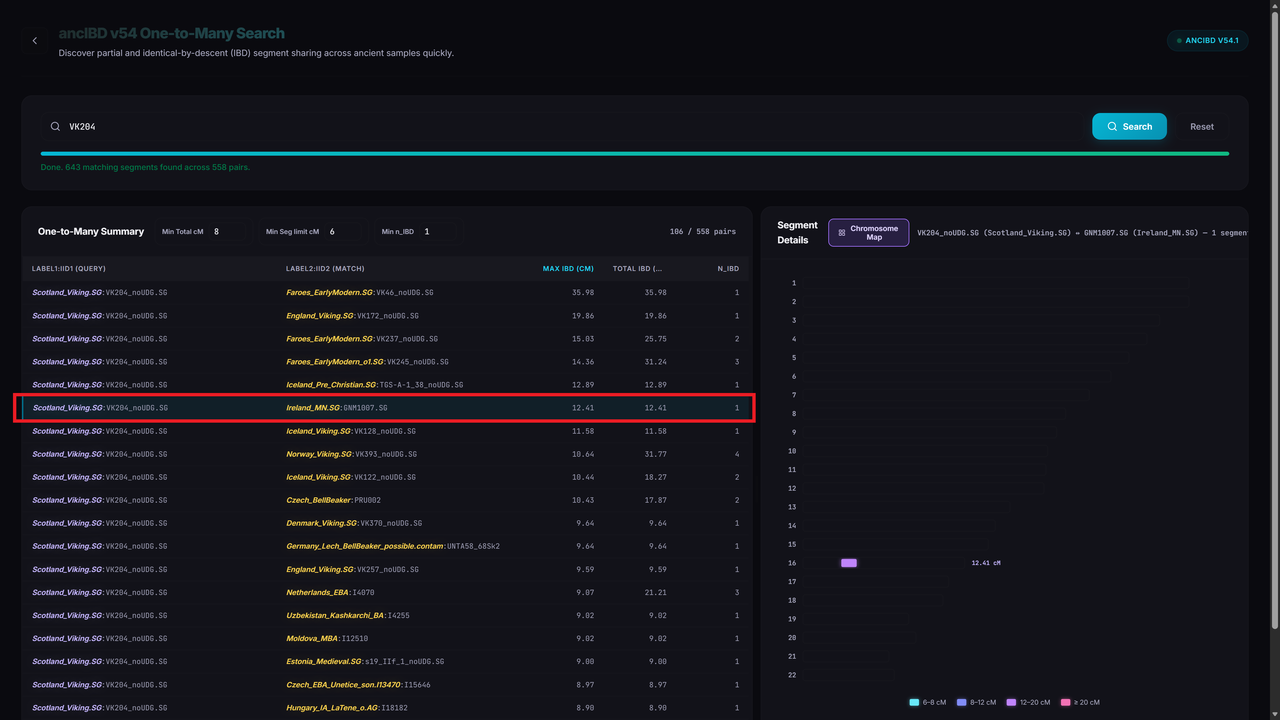
It is a very astute observation. In traditional modern genomics, a **12 cM** segment typically indicates a common ancestor within the last 10–20 generations (roughly 250–500 years). Seeing that same length spanning 4,000 years (roughly 130+ generations) feels like a glitch in the matrix.
However, whether this is a "false positive" depends on how we define the term in the context of **ancient DNA (aDNA)** and the specific mechanics of the **ancIBD** method.
### The Math of Recombination
You are correct about the decay. The probability of a specific IBD segment of length $L$ (in Morgans) surviving for $g$ generations is approximately:
$$P(\text{survival}) = e^{-2gL}$$
For a 12 cM ($0.12$ Morgans) segment over 130 generations, that probability is infinitesimally small. If this were a single, continuous strand of DNA passed down through a direct lineage, it almost certainly wouldn't survive that long.
---
### Why ancIBD Reports These Segments
The authors of the ancIBD paper (Ringbauer et al.) explicitly discuss these "long" segments in ancient contexts. Here is why they appear and why they might not be "false" in a technical sense, even if they aren't "recent" in a genealogical sense:
1. **Haplotype Background & Low Diversity:** In populations with low effective population size ($N_e$) or bottlenecks—common in Neolithic and Bronze Age Europe—certain "ancestral" haplotypes can persist. If two individuals happen to carry the exact same ancestral chunk that hasn't been hit by a recombination event in either of their lineages for a long time, it will appear as IBD.
2. **Imputation Artifacts:** ancIBD relies heavily on **imputation**. aDNA is often "low coverage," meaning we have lots of missing data. To fill the gaps, the software uses modern reference panels. If the reference panel is biased or doesn't perfectly represent the ancient population, the imputation process might "smooth over" small variations, artificially stitching smaller segments together into one 12 cM block.
3. **Ultra-Deep Time IBD:** The paper notes that while IBD is usually for "recent" kinship, their HMM (Hidden Markov Model) can pick up **Background IBD**. These are segments that are identical not because of a great-great-grandfather, but because the population was so small 4,000 years ago that specific segments have simply "locked in."
### Discussion in the Literature
The ancIBD v54 results and the underlying methodology address these concerns in a few ways:
* **False Positive Rates:** The authors acknowledge that at low coverage (e.g., <0.1x), the false positive rate for segments >8 cM increases. If your Orkney or Neolithic samples have low coverage, the 12 cM hit is much more likely to be an imputation artifact.
* **The "Long Tail":** There is a documented "long tail" of IBD sharing in West Eurasia due to the massive population turnover and subsequent bottlenecks during the Neolithic and Bronze Age transitions.
* **Segment Length Thresholds:** Most aDNA researchers treat anything under **10–12 cM** in ancient contexts with extreme skepticism unless the coverage is very high (>1x).
### Is your specific result a false positive?
It is likely a **"statistical" IBD** rather than a **"genealogical" IBD**.
While the two individuals likely do share a common ancestor, that ancestor probably lived much further back than the segment length suggests, and the 12 cM block survived through a combination of population bottlenecks and/or the limitations of the imputation model used by ancIBD.